More on that partnership: I truly believe that offers have been put on the table. However, the company has already gone through Big Pharma partnerships once, so why wouldn’t it succeed again with a targeted genetic population and a stronger effect.
The company has been able to take the drug to Phase 3 alone and knows the drug works, so it’s not worth giving away the risk premium to external parties too early and too cheaply before Phase 3 results and their own GMP license. So, a partnership agreement hasn’t been made, but I think this is a conscious strategic choice made by 2018 at the latest, when the company decided to invest in its own factory, showing that the company wants to control production and the supply chain itself.
If the company also invests in a factory and has organized its drug packaging logistics next door, it provides significantly more leverage for partnership negotiations. But if the pieces fall into place, could they try to take it even further?
The U.S. pharmaceutical market is such an insurance mafia that to get treatments through, a Big Pharma partner is almost certainly needed for marketing (i.e., lobbying insurance companies).
A small part of me, however, hopes that Diamyd could show the middle finger to this system and take advantage of the visibility brought by Orphan Status and success, existing patient networks, and TrialNet clinic connections, and push into the market without a “big brother.” That’s why I was happy when Ulf recently mentioned, in passing, for the first time the possibility of going to market themselves.
No idea what this would cost, but there is cash for several years of “idling” if the TO5 warrant subscription is fully met. At the same time, Phase 3 costs will decrease after 2026. Also, the certification and internal validation of GMP production facilities have certainly generated expenses.
The road to market would probably not be easy. +Advantage, however, is that this is not a daily treatment; a small number of specialist clinics is sufficient.
+The necessary logistical network and production capacity are moderate. The amount of substance required is in nanograms, and when packaged, the entire treatment is three vials. Even at this stage, the facilities set up by Diamyd themselves are capable of producing 36,000 doses per year, and further scaling is likely possible.
+Fast Track and Orphan Status provide a direct line to health authorities in the permit process, and there’s no need for a Big Pharma “fast lane.” Additionally, orphan drug status provides massive visibility.
+Breakthrough T1D is the world’s most influential T1D patient organization, with lobbying and marketing power as well as patient networks. BTD1 has actually participated in Diamyd’s funding round, and as part of a grant program, Diamyd has promised them a “small royalty.” The organization therefore also has financial incentives, in addition to patient advocacy, to get the drug to market.
+Side effects are non-existent, which facilitates insurance coverage.
-Three injections do not stop the disease entirely but slow it down. Is the clinical added value relative to the price sufficient for insurance companies?
-A sales network is needed both to sell to clinics and to negotiate with insurance companies. My understanding is that the network must practically consist largely of healthcare professionals, which is an expensive endeavor.
-The gene-specific target group complicates distribution. Genetic tests are needed for every potential patient. On the other hand, the doctor doesn’t have to guess if the drug works; the genetic test shows it.
-A subsidiary is also needed in the US… Except one has already been established. In the latest presentation, it was mentioned that the company already has several employees in the United States. It’s likely a small outfit for now. In the long run, however, one could assume that production is needed directly in the United States. Tariffs might also affect this.
-No idea what it costs, but surely a lot. In a good case, they reach the market early with their own production, and even if penetration is small, expansion could be carried out with their own cash flow.
@Junkbondking, since you asked for some bear points, here are a couple.
So the company itself estimates peak sales of over 2 billion dollars based solely on that “launch indication” and solely in the United States. Then expansion into the LADA indication another 2 billion. On top of this, the rest of the market, which is presumably at least the same (EU, Asia, S. America, etc.)… let’s say 2 billion…
This makes 6 billion, and if you throw in some very moderate multiple, this is a 10 billion+ company.  Plus their own factory, thanks to which margins are huge. And a huge number of patents and like a ten-year exclusivity to sell this drug to people all over the world.
Plus their own factory, thanks to which margins are huge. And a huge number of patents and like a ten-year exclusivity to sell this drug to people all over the world.
That $2B peak sales is calculated at approx. 60k patients with 80% penetration and 30% coverage at a $150k price. In my own gut feeling, these pharmaceutical company peak sales numbers tend to be pulled out of a hat, and penetration rates like that are outrageously high.
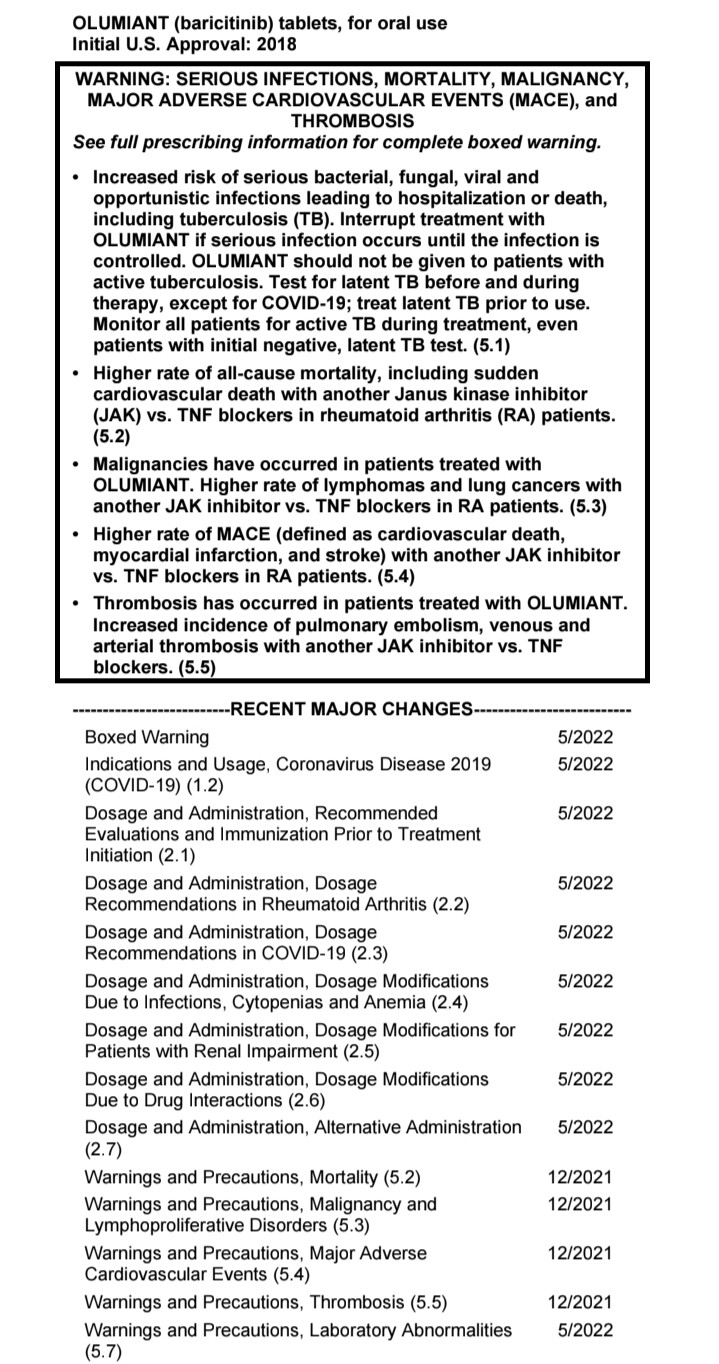
Even though it is an orphan drug, the figure sounds too high for this pipeline. First of all, the estimates probably assume there isn’t much competition. Now Tzield is going to market. Even though it is objectively a worse drug and currently priced at 200k, competition can lower prices. In the coming years, previously mentioned new and old immunosuppressants etc. will likely join, even if they are terrible “poisons.” Secondly, 60k patients is a high assumption, when in practice only 40-50% of the population possesses the correct haplotype and 64k new T1D cases occur annually in the United States. In the early stages, one could theoretically achieve relatively higher penetration as treatment can also be offered to those recently diagnosed, but the benefits of the treatment fade quickly if cells have already been destroyed for a couple of years, and I don’t believe late-started treatment would easily pass through insurance companies.
If Diamyd ended up partnering in the US, upfront payments would certainly be substantial once Phase 3 is complete. But a large portion of that $1-2B in sales would end up with the partner. A less optimistic person would say that achievable sales in the US are $1B and a partner is needed; from this, 30% royalties would make about 300 million minus costs, but the golden eras can be expected to continue only for a limited time before better and/or cheaper alternatives lower the margins.
Roughly speaking, it seems that typically during Phase 1, a company gets about 5-10% royalty on top of milestone payments. After Phase 2, 10-20%, and after Phase 3, 20-30%. In Diamyd’s case, maybe even more because of own manufacturing and orphan drug status, but still, the biggest pile goes to the partner.
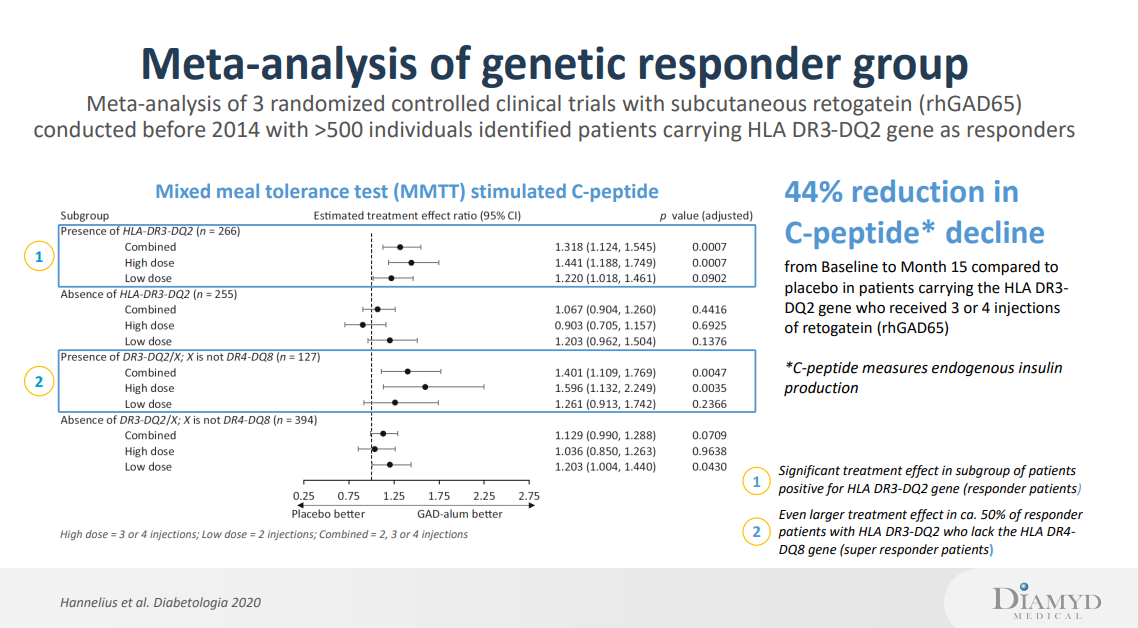
If, on the other hand, Diamyd aimed for the market itself, it would cost a lot of money and would likely still be much slower than with a partner. A problem might also arise from the fact that I assume Diamyd wants to immediately start new expensive studies to expand the indication for use. Stage 1-2 preventive treatment, LADA treatment, and additional boosters all likely require fairly large studies, although not a full research pipeline. Even if they were pushed through, half of the mechanism of action by which Diamyd works is still untapped: If GAD65 works for DR3-DQ2, it’s also worth believing that Diamyd’s patented insulin-based treatment for the DR4-DQ8 haplotype works. This would cover 90% of T1D patients, but there hasn’t been money for the research yet. Funding these is so expensive that Diamyd might inevitably be forced to license part of its portfolio.
In this bear case, I must mention a tongue-in-cheek bull scenario: If everything could be kept for themselves and sales reached half of the estimate, i.e., $1B worth at an 80% margin, it would make Diamyd about a 16 billion value company with a moderate 20 P/E. Solely in the United States and without booster treatments, LADA treatments, and without preventive treatment. And without that DR4-DQ8 haplotype treatment which might double everything previous.The most realistic bull scenario would be licensing and, after a transition phase, contract manufacturing in the United States, whereby the lump-sum payments received from the agreement guarantee funding for other R&D pipelines. The Swedish factory serves Europe, where the rights are retained.