Following up on that:
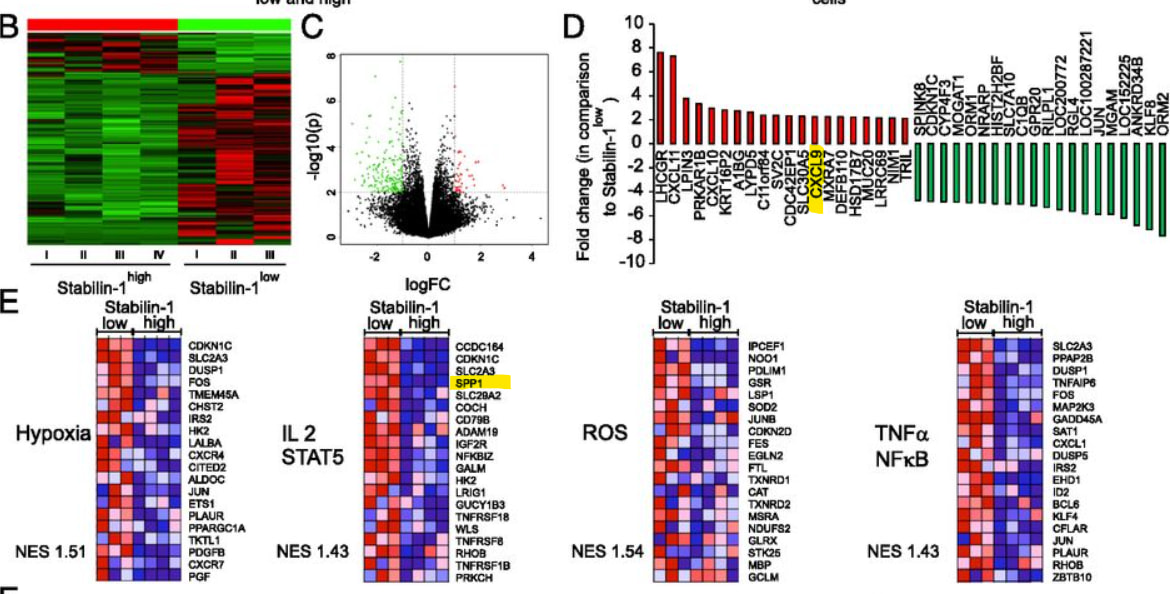
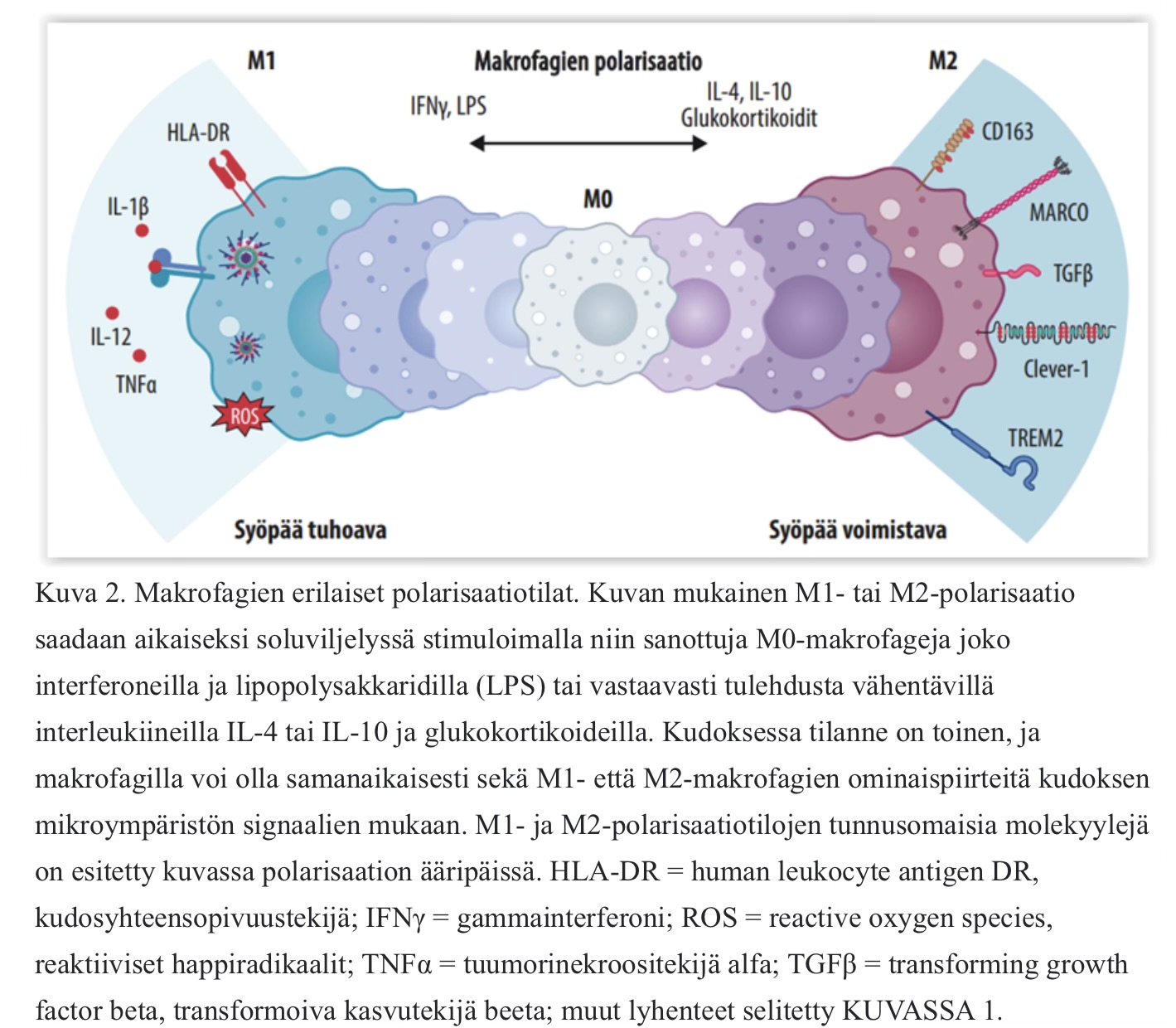
Those SPP1 macrophages are also linked to immunosuppression. So it’s related to Clever-1 positive macrophages at some level. However, there doesn’t seem to be any information on whether the existing mechanism of action, i.e., Bex, would affect that SSP1 pool through some pathway. It’s probably competitive silence, or SPP1 is such a new thing that research data isn’t available yet. They did promise to investigate, “This framework may help identify patients who are more likely to have resistance to immunotherapy and support testing new combination treatment strategies.” Maybe Maija could help?
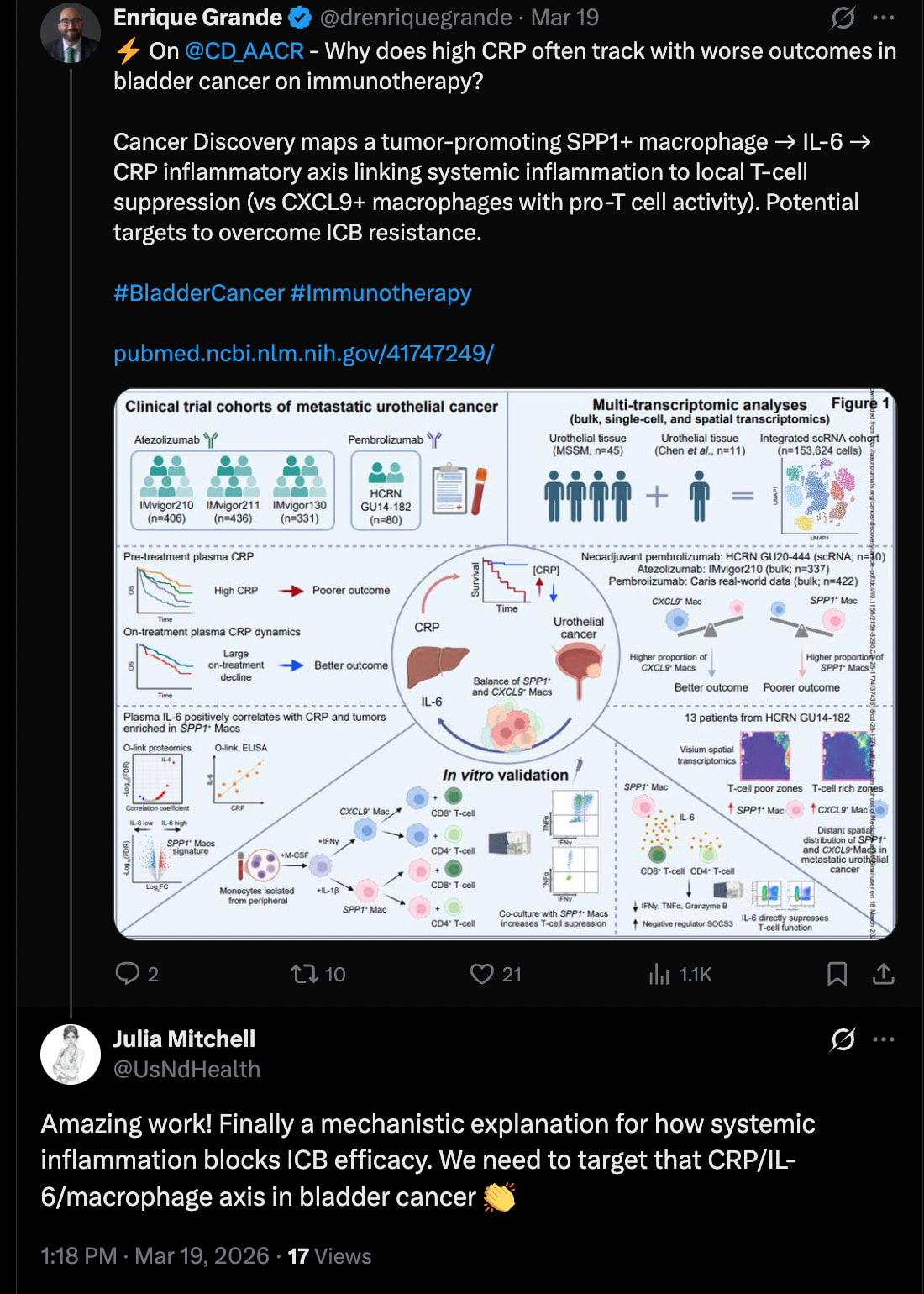
Rannikko, in his dissertation posted in the thread a couple of days ago, also talks about the same thing as the authors of the Mount Sinai CRP, IL-6, SPP1 article; in the latter:
“In contrast, the team identified another type of macrophage marked by CXCL9 (Chemokine ligand 9) that helps activate T cells and is linked to stronger immune responses.”
Rannikko: "Bexmarilimab treatment induced TAMs to secrete CXCL10 ex vivo and upregulated another CXCR3 ligand, CXCL9, in patient tumors.”
And “Several of these bexmarilimab-induced changes also predict better ICI therapy response, such as elevated CXCL9 levels, T-cell infiltration and IFN signaling (Ayers et al., 2017; Herbst et al., 2014). ”
House, I. G., Savas, P., Lai, J., Chen, A. X. Y., Oliver, A. J., Teo, Z. L., et al. (2020). Macrophage-Derived CXCL9 and CXCL10 Are Required for Antitumor Immune Responses Following Immune Checkpoint Blockade. Clin Cancer Res, 26(2), 487-504.
CRP and IL-6 in the blood are also indicators of general inflammation in the body. Rannikko suggests instead of them as biomarkers, "patients with low Immunoscore, PD-L1 and IFN score would be non-eligible for ICI therapy and eligible for bexmarilimab therapy.”
Immunoscore is a T-cell measurement of a cancer sample that shows whether immunity is active. ICI therapy here means, for example, pembro, those that have not been effective in melanoma and lung cancer in the BLAZE trial. PD-L1 score indicates how likely those pembros and zimbets etc. would work. IFN-score is a measurement of the activity of interferon-stimulating genes, also an inflammation indicator.
It will be interesting to see what is selected for BLAZE and whether those will be tested in it, and what will be selected for continuation. It seems that biomarkers would best identify those who respond to Bex.