Help is on the way. The challenges of MDS trials are now featured in the Expert Review of Anticancer Therapy publication:
Zeidan himself says this is his 400th peer-reviewed article. Not bad for a scientist who isn’t exactly at retirement age yet. Other authors include oncologist Stahl from Yale, Huttunen as a statistical health economist, and staff from Faron.

The thread already featured a Blood publication on the topic “The Conundrum…”
In this one, Zeidan writes that researchers shouldn’t wait for a “miracle drug” that doubles survival time all at once, but rather focus on smaller, yet significant, steps forward.
Because: With current treatments, patients’ life expectancy tends to plateau at around the two-year mark; crossing this threshold is difficult.
Selecting patients for the study based on specific genetic mutations so that the treatment hits the right target and results are clearer—i.e., molecular enrichment. Or then stratification (as the phase 2/3 was intended to do regarding TP53).
Research must be adaptable on the fly based on results so that resources are not wasted on ineffective drugs. (As the phase 2/3 was intended—meaning the sample size can be adjusted according to results, a “seamless design 2/3” (which is apparently being abandoned), and Z. says that it must be possible to stop useless ones).
Additionally, it must be managed and predefined how those proceeding to stem cell transplantation are handled, as well as those receiving other drugs after the study (that Vene [Venetoclax]!).
I’m sure BEXMAB-2 will still turn out to be valid. That is, in a way that demonstrates the efficacy of Bex+aza without the pitfalls of study designs undermining the potential.
Zeidan has communicated in Faron’s webcasts that he has buried numerous MDS drug hopes, and now his eyes have apparently opened properly after the Verona trial; the ambition now is to actually get something through, but in a different way.
Some might remember this image from over a year ago. I added the latest one to the image.
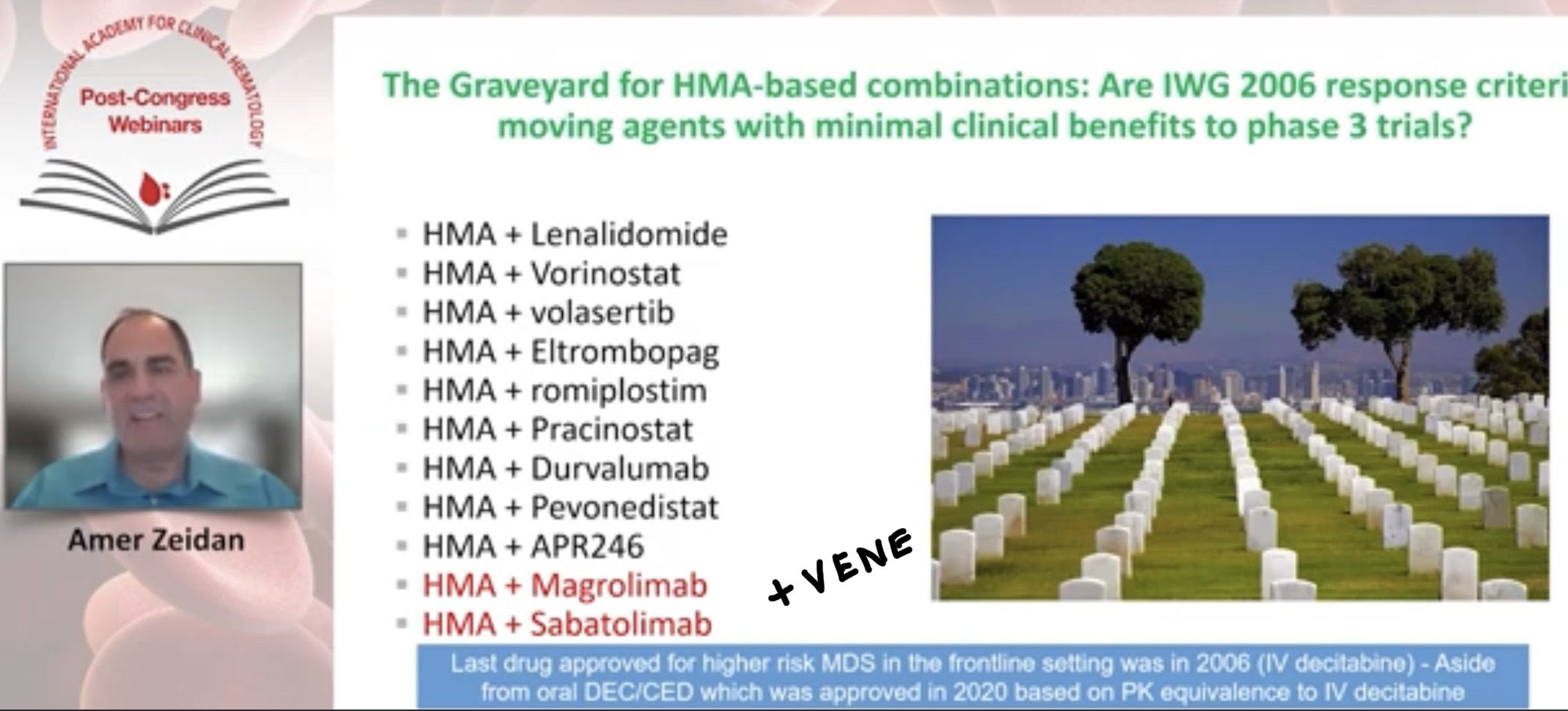
IWG2006 was blamed there. Then Zeidan and his group developed IWG2023 and, from those criteria, for example, cCR, which was already accepted at the FDA’s EOP2 meeting as a secondary endpoint for Phase 3. The FDA does listen to scientists, but there is still some work to do—though it’s better to do it now than after the fact.