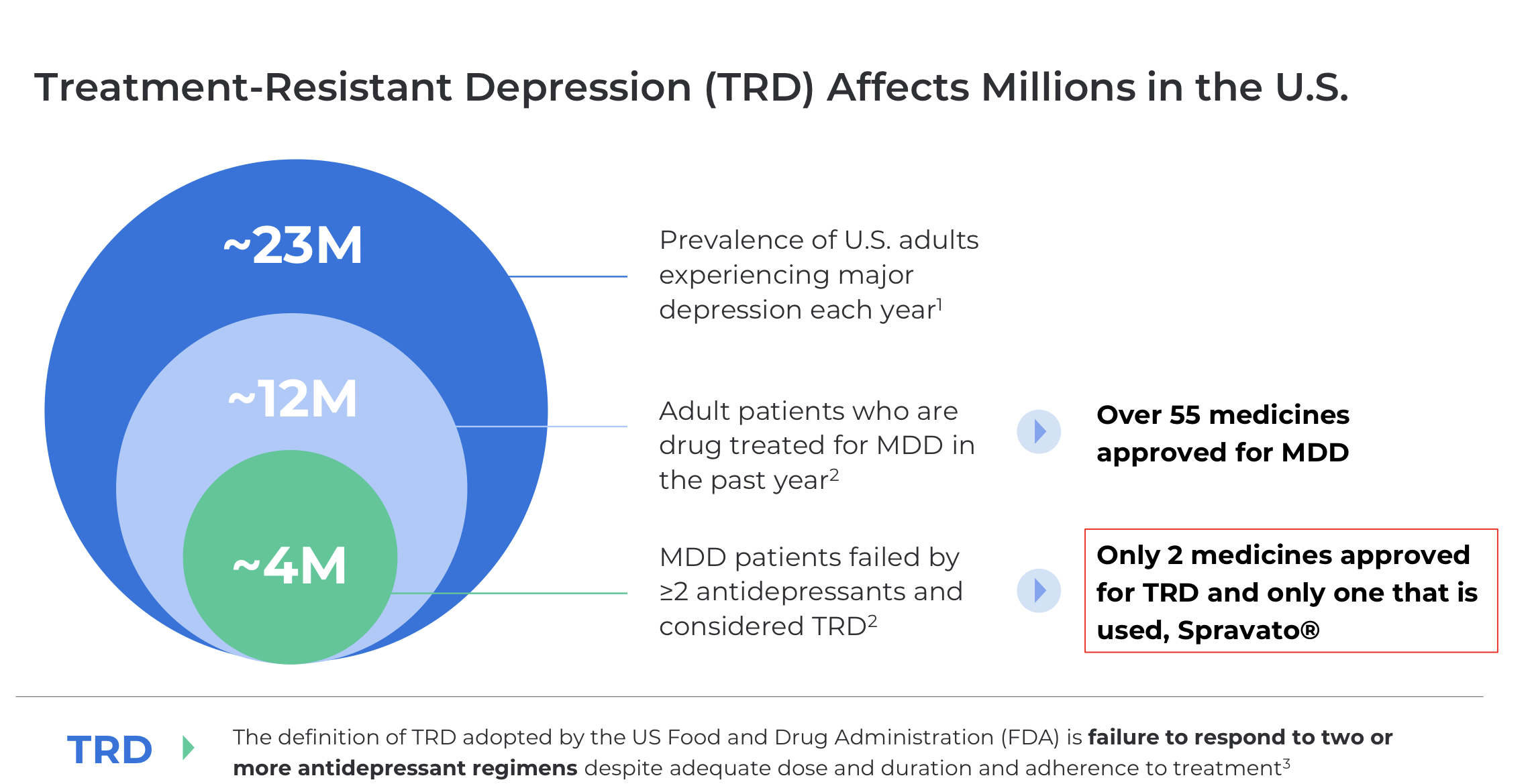
Compass Pathways is a UK-based biotechnology company developing COMP360 psilocybin therapy for treatment-resistant depression. What is treatment-resistant depression? It is a form of depression for which current drug treatments work poorly. In the United States alone, we are talking about a market of millions of patients:
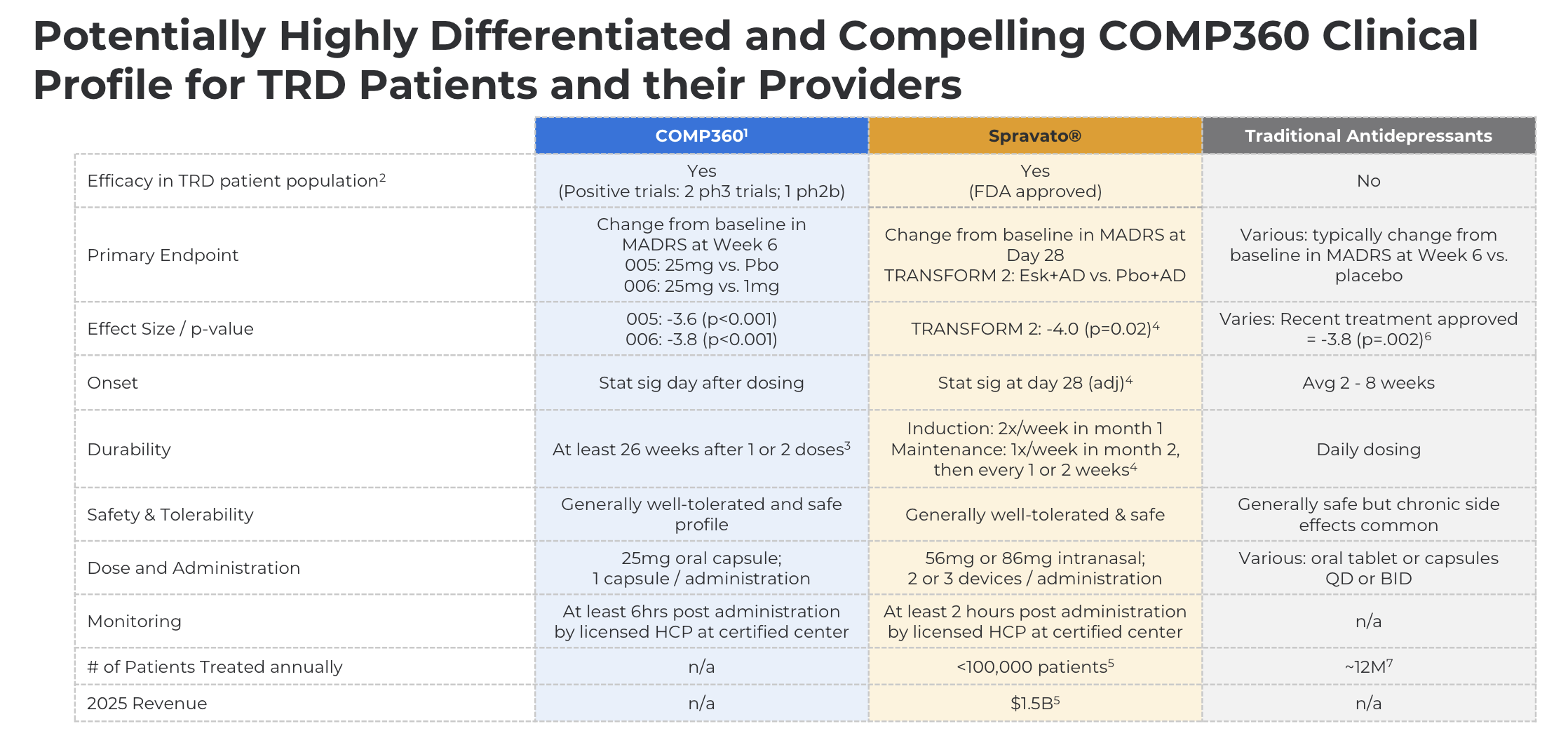
In practice, only one effective drug is available to millions of patients in the US, Spravato (developed by J&J), the use of which is impractical as it requires the patient to visit a clinic once or twice a week and spend several hours there. With COMP360, the same patients can be treated much more conveniently because the depression treatment can be administered in just one or two doses, giving the drug a huge competitive advantage:
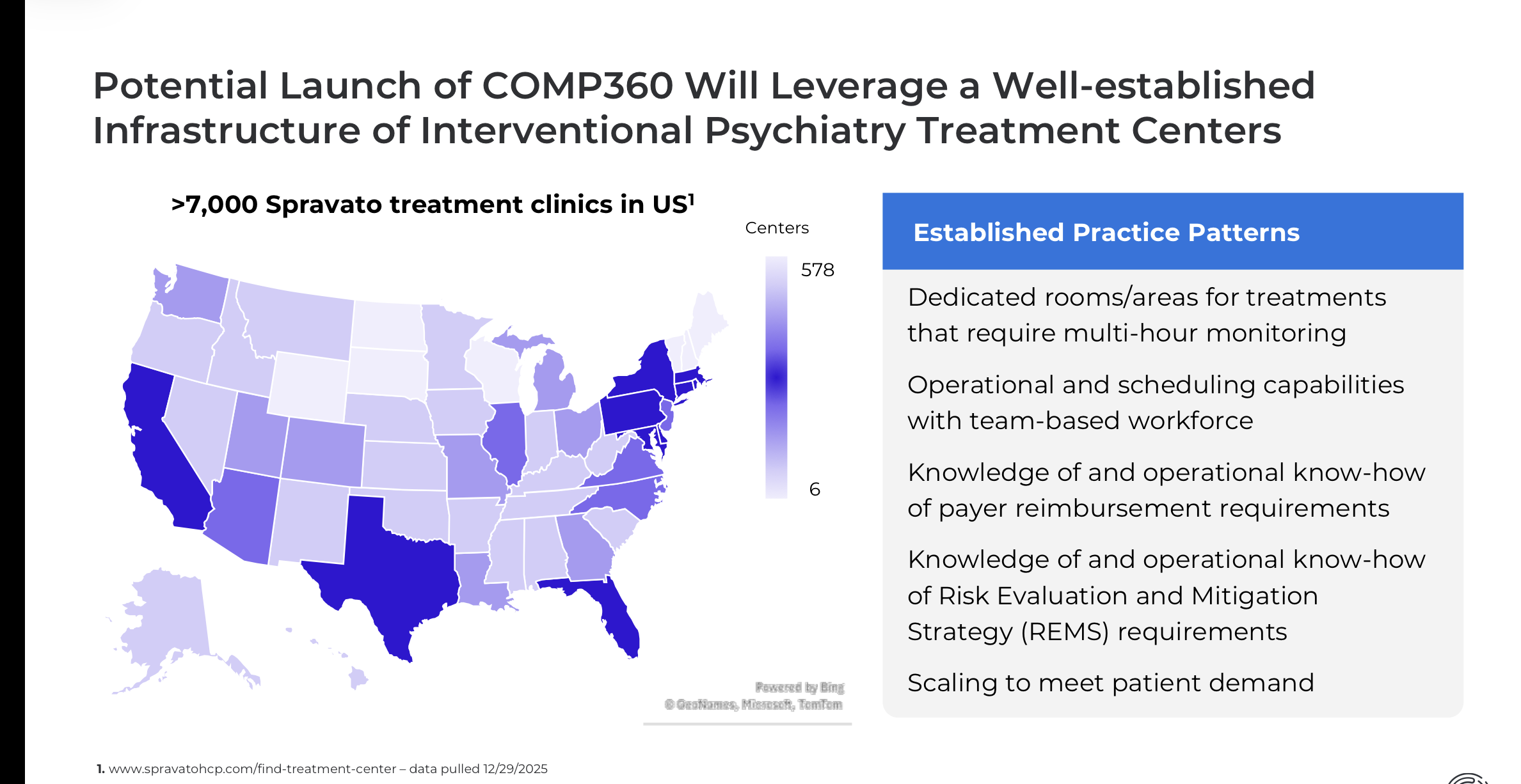
Because this drug requires clinical monitoring and the business logic therefore differs from conventional medications, Compass’s sales strategy is to target the same clinics where Spravato is already being used and where infrastructure and expertise for monitoring patients for several hours after administration already exist. Thus, Spravato did the hard work of paving the way for Compass, and now that same path is intended to be used for faster scaling:
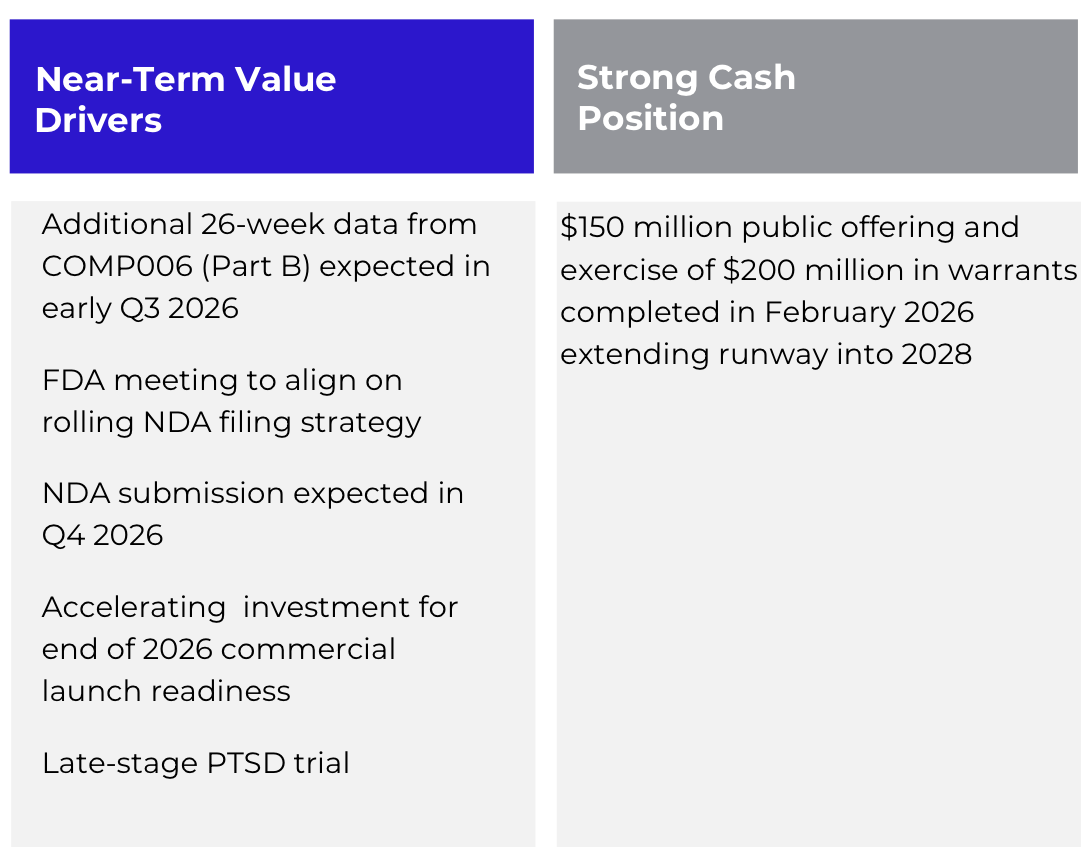
Things have progressed quite well in the sense that Phase III Part A has already been successfully completed and the drug proven effective at the 6-week mark. Now, we are still waiting for Phase III Part B data at the 26-week mark, which is expected to be completed during Q3 2026. Unless there are unexpected health risks or other exceptional results, a New Drug Application (NDA) can be submitted in Q4 2026, clearing the way for commercial operations in 2027. There is enough cash in the bank for the next couple of years, and the pipeline also includes an expansion of the drug’s use for the treatment of PTSD, with results expected in the coming years.
Joe Rogan and other American influencers have recently given the entire sector significant momentum, as President Donald J. Trump issued a high-profile executive order to promote the use of psychedelic drugs for the treatment of mental illness. Since Democrats also view psychedelics positively, political risks regarding these sensitive treatments are now lower than ever in U.S. history:
One important question that these slides don’t directly answer is how they’ve accounted for the fact that subjects can easily tell if they are receiving the drug vs. a placebo, specifically due to these very distinct side effects of psychedelics (especially hallucinations). This is a widespread issue that has only recently started to receive attention in psychedelic research (see e.g., https://jamanetwork.com/journals/jamapsychiatry/article-abstract/2846479).
Professor of Psychiatry Erkki Isometsä actually lectured us on this a short while ago at work and highlighted that exact problem. I can’t for the life of me find the specific study he was referencing right now, but the message is the same: based on current data, the efficacy of psychedelics in treating TRD does not differ from traditional antidepressants, and sometimes the efficacy is even lower. The question regarding Compass Pathways is surely how they have tackled those traditional problems related to the study and blinding of psychedelic drugs.
Regarding Spravato, a quick word in the Finnish context: its price is so outrageous (in the HUS region, around €13k per single treatment session for one patient) that it is not used at HUS at all, for example, because neuromodulation units already exist with the staff and infrastructure in place to administer IV ketamine, which is even more effective than i.n. ketamine (Spravato).
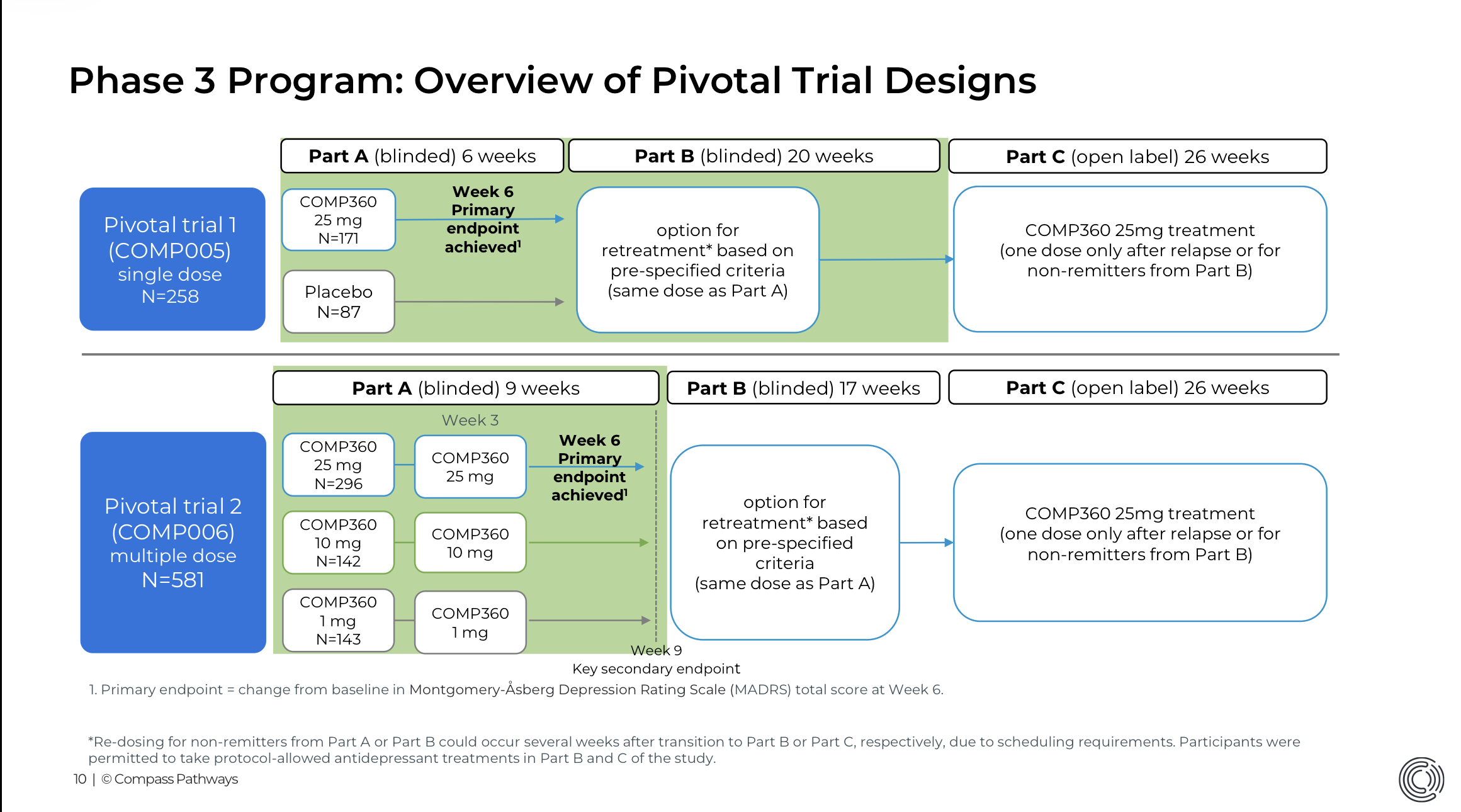
That’s a great point! In its studies, Compass has tried to tackle this with high-dose vs. placebo and high-dose vs. low-dose designs (25 mg vs. placebo and 25 mg vs. 10 mg vs. 1 mg), meaning several Phase III designs are running simultaneously.
At 10 mg and 1 mg doses, effects already occur, so the patient cannot be entirely certain whether they received a high or low dose. As I understand it, this is an FDA-approved trial design for psychedelics
So nothing can stop the money from rolling in if the drug starts displacing Spravato?
This setup tackles the issue well indirectly, but there’s still likely a problem in that when the patient knows they are receiving the investigational drug (even if the reality is they only get a small dose), it probably has some impact on the treatment response. A larger-scale problem arises here because, as far as I know, we don’t have any estimate of how the placebo response varies as the dose decreases. It’s certainly a good educated guess that the decrease in placebo response probably isn’t linear, for example, but what the exact response curve is for the placebo remains a mystery.
It’s very possible that if marketing authorization is granted by the FDA and they enter the market, they will definitely capture some market share from Spravato. Estimating the exact potential is no longer such an easy exercise, but I’m sure someone can whip that up too.
As we are tackling treatment-resistant depression here—defined as two or more previous antidepressants failing to work—you would think that seeing any effect in the statistical data would be a major achievement in itself. I mean, if standard antidepressants don’t show a difference from placebo in these patients, then achieving any significant separation from placebo should be meaningful. The bigger question is whether they can generate enough benefit and differentiation compared to ketamine, which is currently the best treatment for these toughest cases. The durability of the drug’s effect after just a few sessions is critical, as the competitive edge relies specifically on requiring significantly fewer visits than ketamine treatment
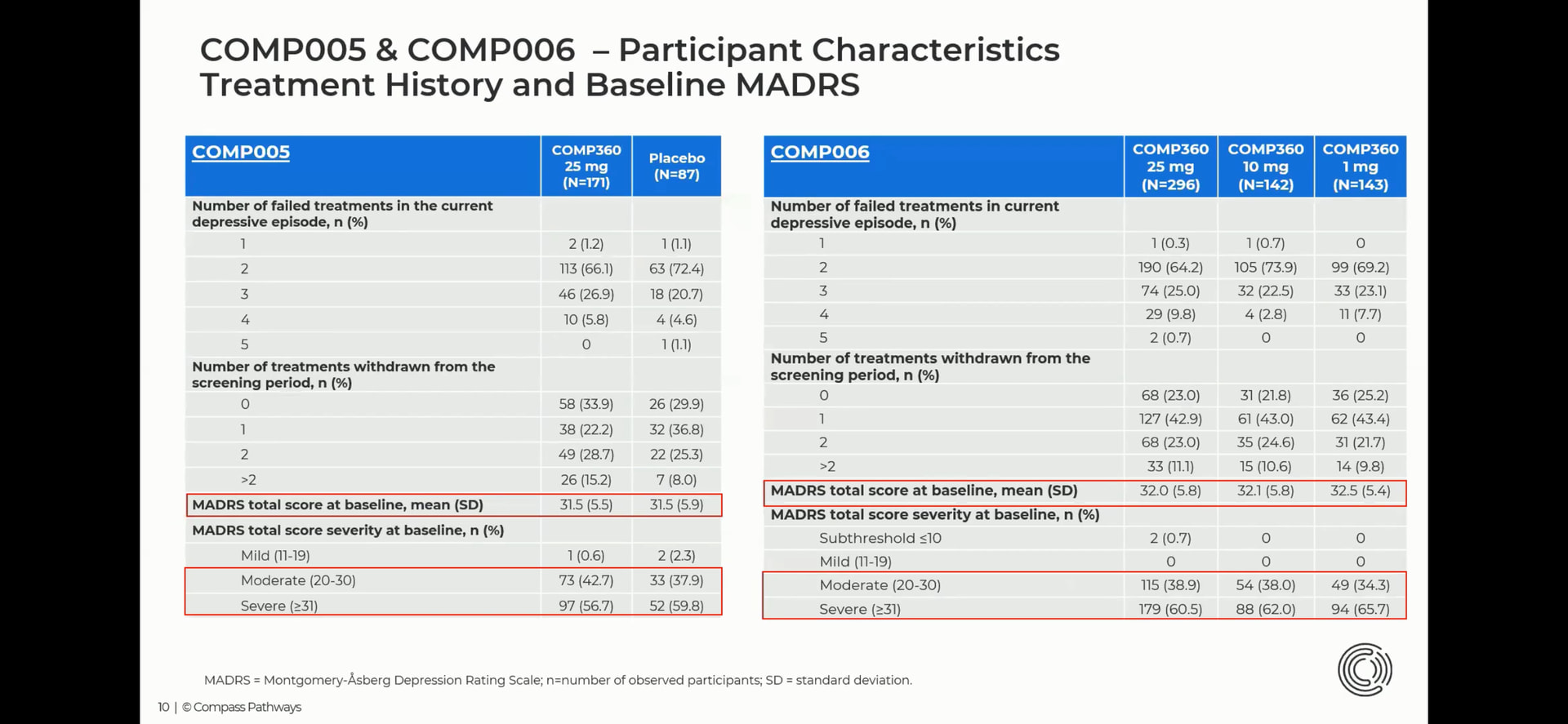
It’s important to remember here that the studied populations are not directly comparable. First of all, as Pohjolan Eka also mentioned, these are specifically patients for whom antidepressants have not provided any benefit. Here is more detail on the patients from both Phase 3 trials:
Don’t these look like quite severely and treatment-resistantly depressed patients?
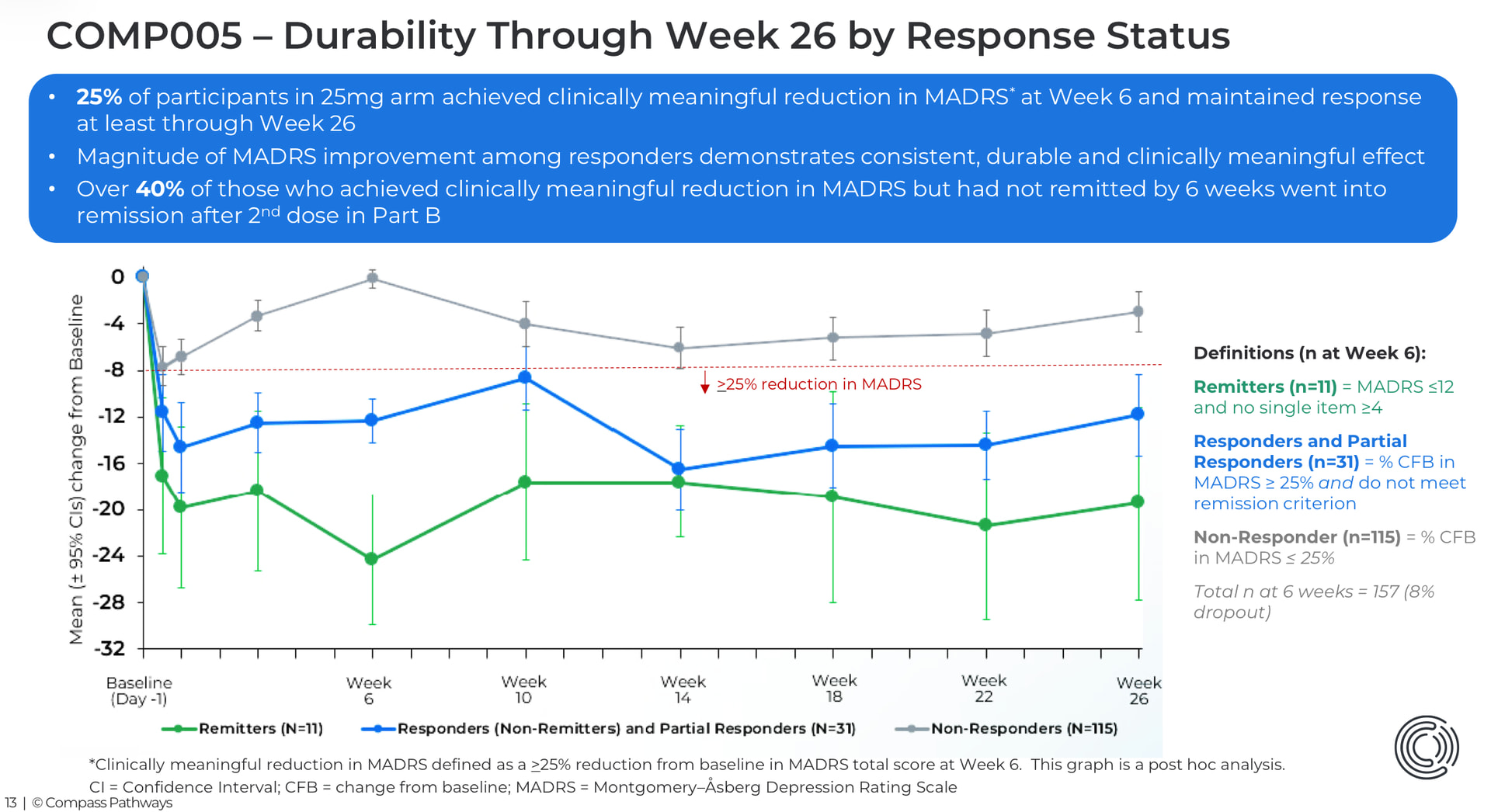
The MADRS reductions compared to placebo—the “delta”—are roughly in the same range as with Spravato. In my opinion (based on AI analysis), slightly larger than with traditional antidepressants (meaning the efficacy of psychedelics in TRD is better than SSRI/SNRI in MDD, not TRD, which is a more difficult patient group to treat). The remission percentage in studies also depends on the baseline MADRS level, if remission is defined as MADRS below a certain score—was it 10 or something like that. So if the baseline MADRS is high, it’s harder to achieve remission. For example, in Spravato studies, if I recall correctly, the remission percentages were better, even though the MADRS drop was roughly equivalent.
So, Johannes, are you a psychiatrist?
I recently listened to a podcast where Isometsä was a guest. To me, his attitude toward these treatments sounded very unenthusiastic. Besides being professionals, we are also humans, and things other than pure data can easily influence which information we emphasize. In my view, it is scientifically possible to justify both a critical and a positive/enthusiastic stance toward these treatments in light of current data.
I really have to defend Isometsä here. For example, the following piece by him from 2024 is a very balanced description of the situation at that time (bolding mine):
Psilocybin is the most studied psychedelic in the treatment of depression, with strong neuroplastic and neural network integration-enhancing effects (13). These have been speculated to enable the formation of new associative connections. Several controlled studies on psilocybin have now been published in top medical journals (14-16). It is starting to look clear that a single dose of psilocybin in conjunction with an intensive psychotherapeutic treatment session produces significant benefit for at least some patients suffering from very chronic and severe depression. The proportion of patients achieving a treatment response in these studies has been 37–70% (14-16). In new studies, however, some patients have also shown significant adverse effects, long-term deterioration of clinical status, and increased suicidal ideation (16). Non-professional behavior by therapists has also been reported in connection with the psychotherapeutic support provided during psychedelic and MDMA treatment sessions, to which the patient’s exceptional state of mind during the treatment session likely predisposed them. The research base for the therapeutic use of psilocybin is still narrow, there are still significant methodological flaws in the studies, and the safety of the treatment is not yet clear. At the time of writing, the therapeutic use of psilocybin is permitted under special conditions in Australia and Switzerland.
Just a few years ago, there was considerably less evidence, and the harms were emphasized in a completely different way and in a rather moralistic tone, but now that evidence is starting to emerge, the benefits simply must be acknowledged. Psychedelics are partly a generational issue, as Finns have very strong prejudices against these substances, and of course, a person cannot escape their society and upbringing; however, there is such a desperate shortage of effective depression treatments and new PTSD medications that these will eventually be adopted if/when there is no better alternative.
I agree, that is written quite neutrally. In the podcast I mentioned, it could of course be that he ended up in a sort of opponent role due to the conversational dynamics, as the other participant (Hupli) is clearly enthusiastic about these therapies. But in the podcast, his attitude sounded very critical; I got the impression of a ”dismissive” attitude
Regarding Hupli, it should of course be noted that he has been exceptionally close to Compass Pathways’ research and has also been actively experimenting himself, so without questioning anyone’s professionalism, there could naturally be a bias in a positive direction. For example, here are a few excerpts from the Hesari article:
Finland naturally won’t be adopting these, since “oh how dreadful, a doctor giving patients hippy drugs,” but fortunately, in America, these things are viewed more permissively and productivity is in a completely different class, so there is also the means to pay for expensive treatment.
I’d like to continue a bit more on this efficacy issue.
First, if you’ll allow me to nitpick the wording, TRD refers to Treatment-Resistant Depression, which by definition means depression that traditional antidepressants don’t work on, so conceptually there is a contradiction in this sentence. (Well okay, the term refers to depression where two antidepressants have been tried without response; it could be that a third attempt or augmentation would still produce a response even if it was already defined as TRD before that.)
I personally think that this MADRS reduction and the “delta” is an especially relevant tool specifically for obtaining marketing authorization from drug authorities. When considering SSRIs, for example, they received their marketing authorization with this kind of evidence, but once efficacy has been demonstrated and the license granted, MADRS reductions aren’t really considered in clinical work or for individual patients—at least it’s not the most essential factor in assessing treatment efficacy or determining whether the started treatment is working, or if the dose needs to be increased or the drug changed. It’s enough if the patient feels sufficiently relieved and is happy to continue the medication, or maybe eventually ready to stop. At the primary care level at least, this is how it goes, even if someone might ask for a GDS (Geriatric Depression Scale) for more than just screening purposes? (You can probably say better how it is in psychiatry.)
So, after obtaining permits, in clinical work: if patients feel they have benefited from these therapies, we can say the treatment works. At that point, utilizing the placebo effect (or the care/treatment effect) is permissible and even desirable.
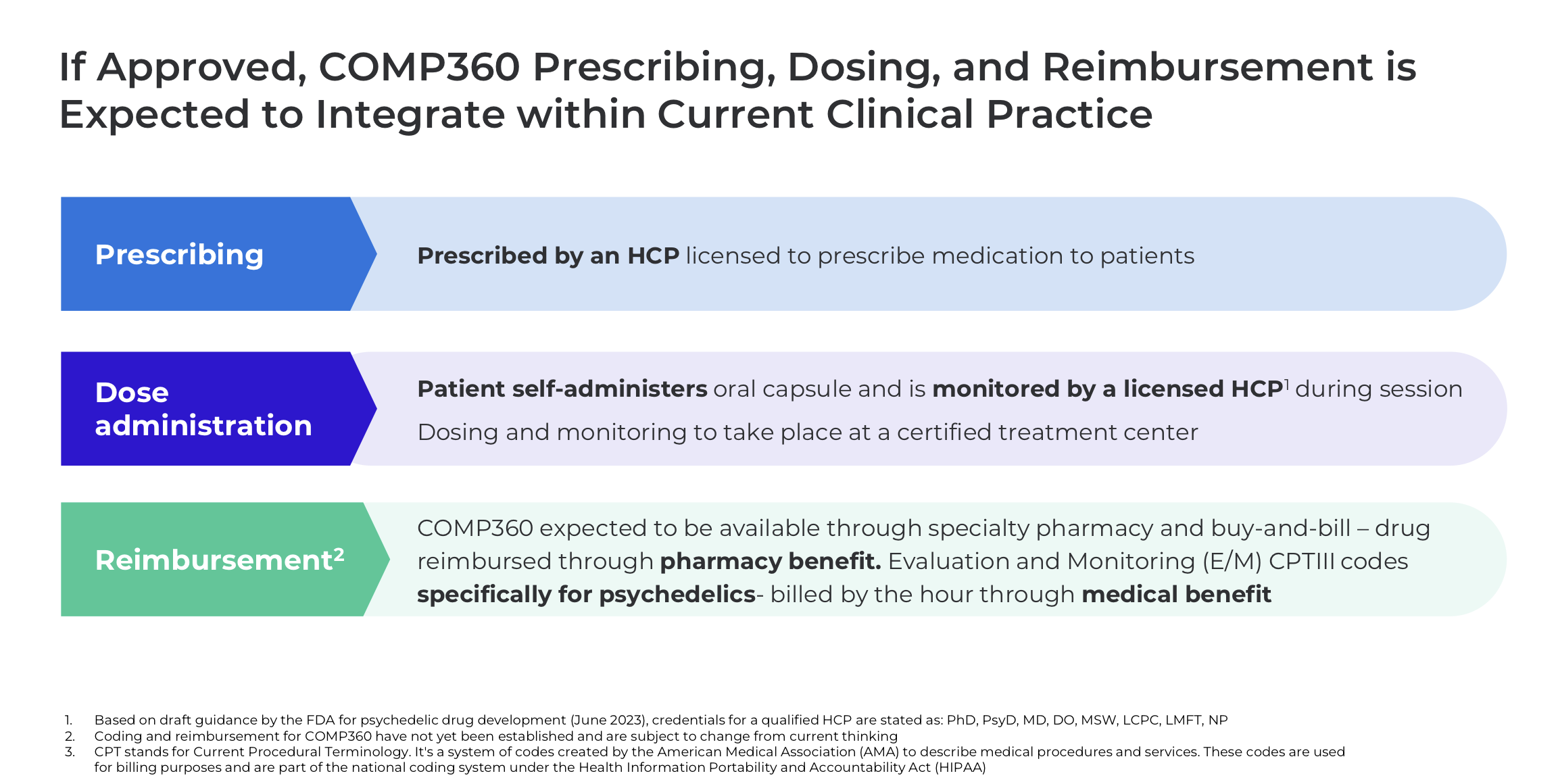
Some experts have pointed out that the observed efficacy in current studies (like Compass’s) might be lowered by the fact that the role of “psychotherapy” in the psychedelic treatment entirety has had to be removed from the research protocol, especially after Lykos Therapeutics’ CRL (Complete Response Letter) regarding MDMA-assisted psychotherapy for PTSD. This is because the FDA stated that evaluating psychotherapy is not within their field, and it is difficult to separate which part of the efficacy comes from the drug and which from the therapy (especially since “functional unblinding” occurs and affects both patient and therapist expectations). So if psilocybin is thought of as a psychoplastogen, a producer of neuroplasticity, it could be that guiding the patient in the right direction—or at least supporting the found direction—could help, but the possibilities for this in these Phase 3 studies were very limited. After marketing authorization, talk therapy can also be used. (Though it is a separate question to what extent it could be reimbursable if efficacy has been proven specifically without therapy, and considering that therapy is expensive.)
It may also be that all the benefits of the treatment are not reflected only by mood-measuring scales. Many who have undergone a psilocybin session rank the experience among the few most important experiences of their lives. What if the mood doesn’t shift completely out of depression, but the patient still sees their life in a significant new light, and for example, appreciates their own life, daily routine, and relationships with loved ones anew, perhaps approaching their depressive symptoms from a slightly different perspective even if they haven’t completely disappeared?
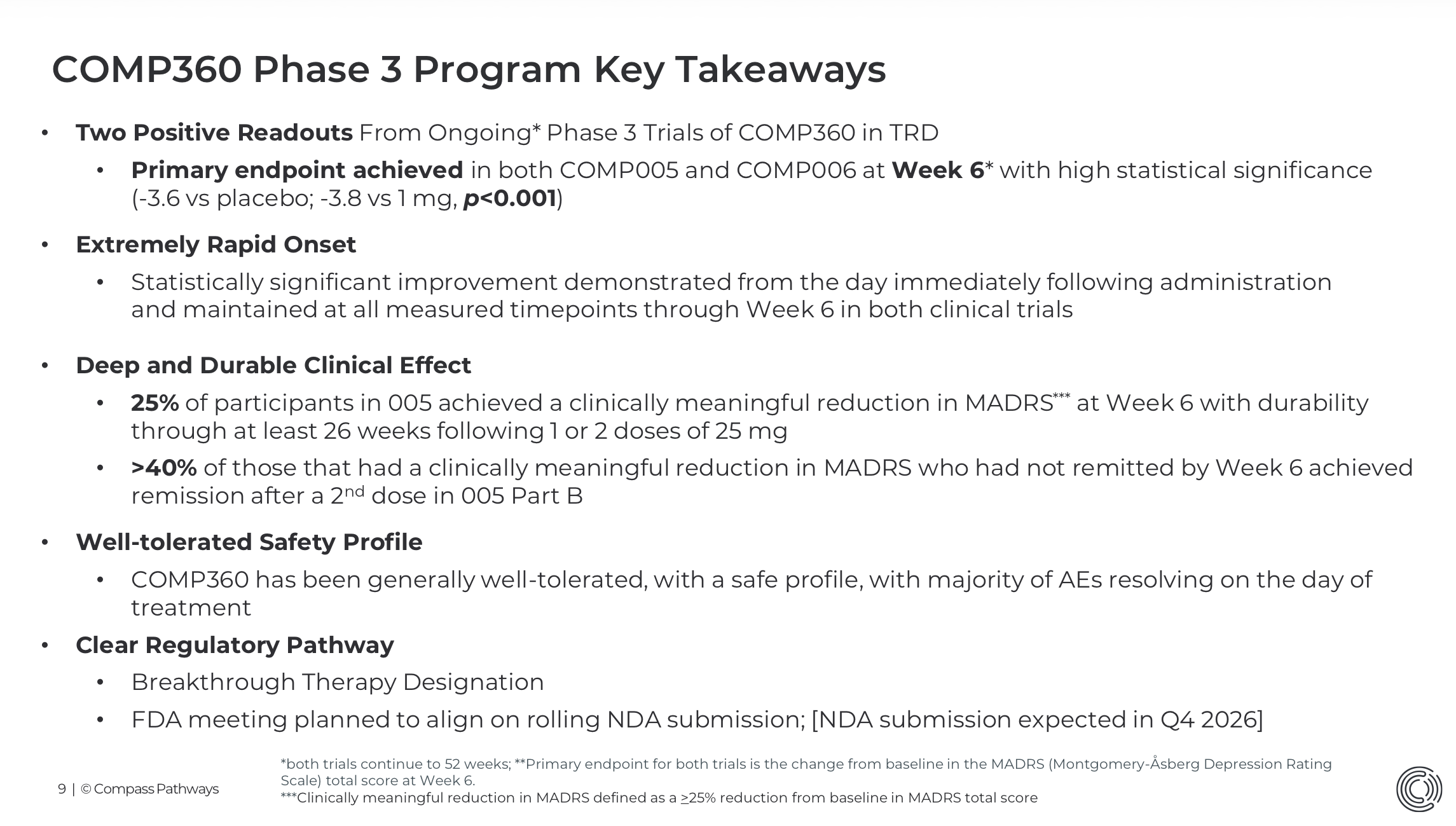
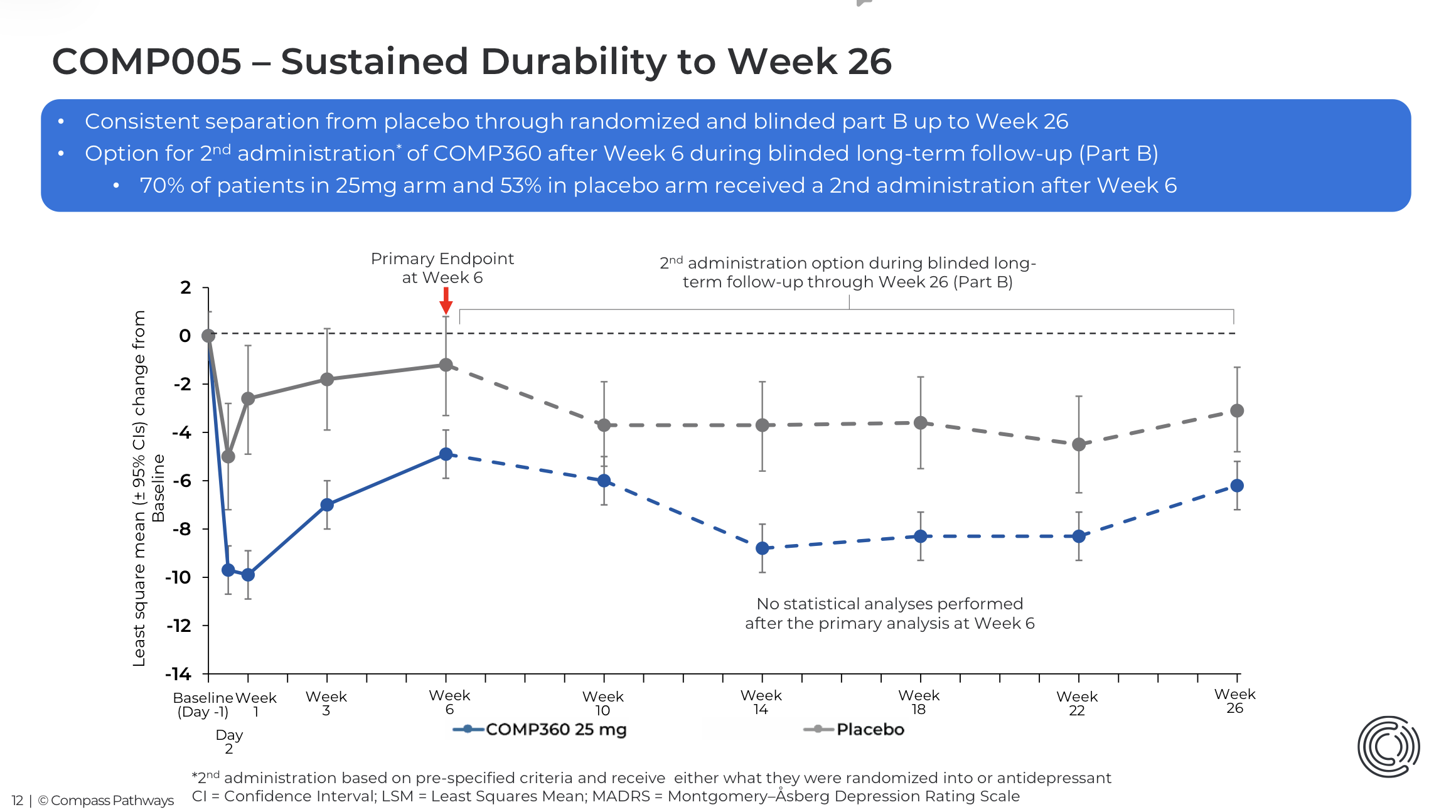
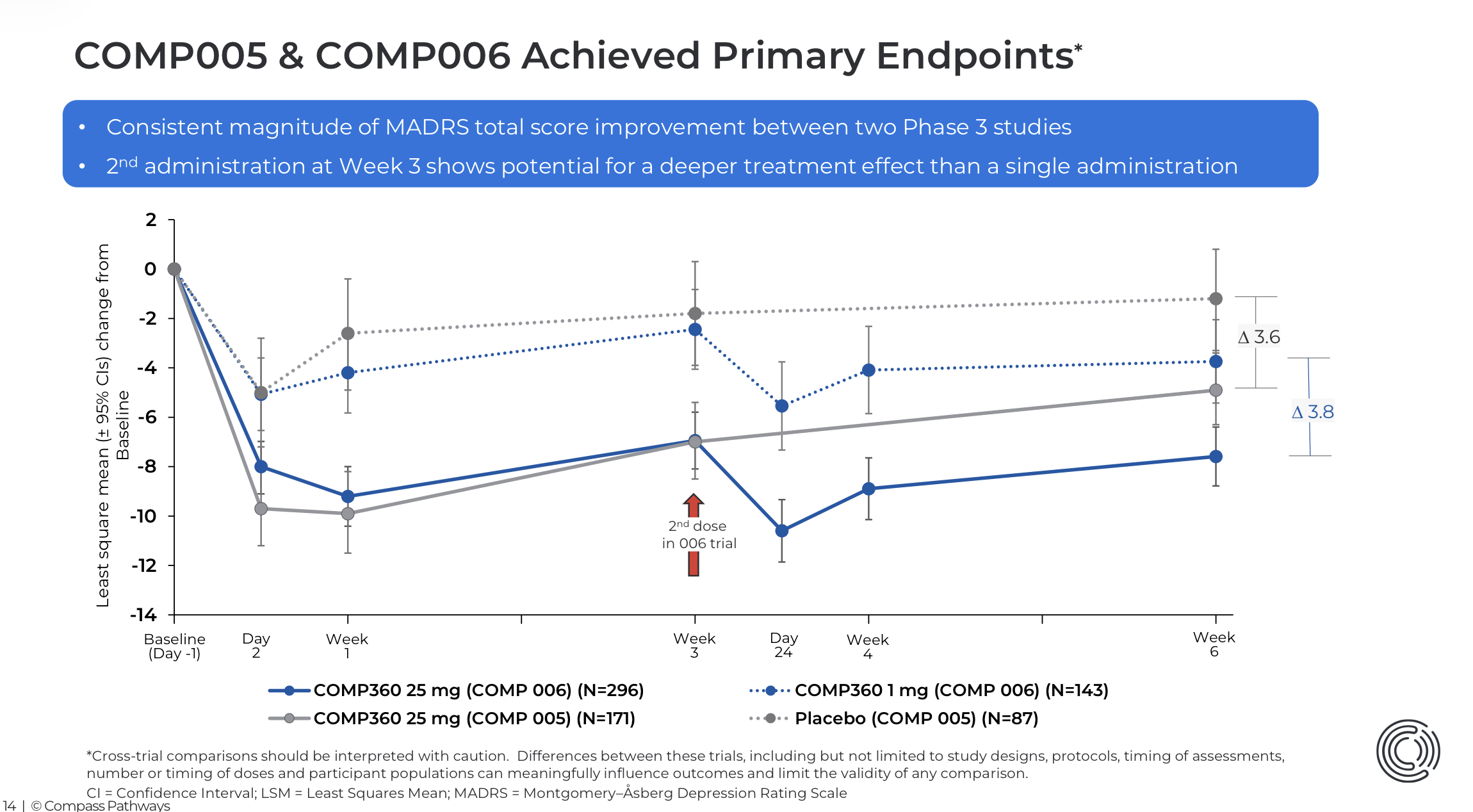
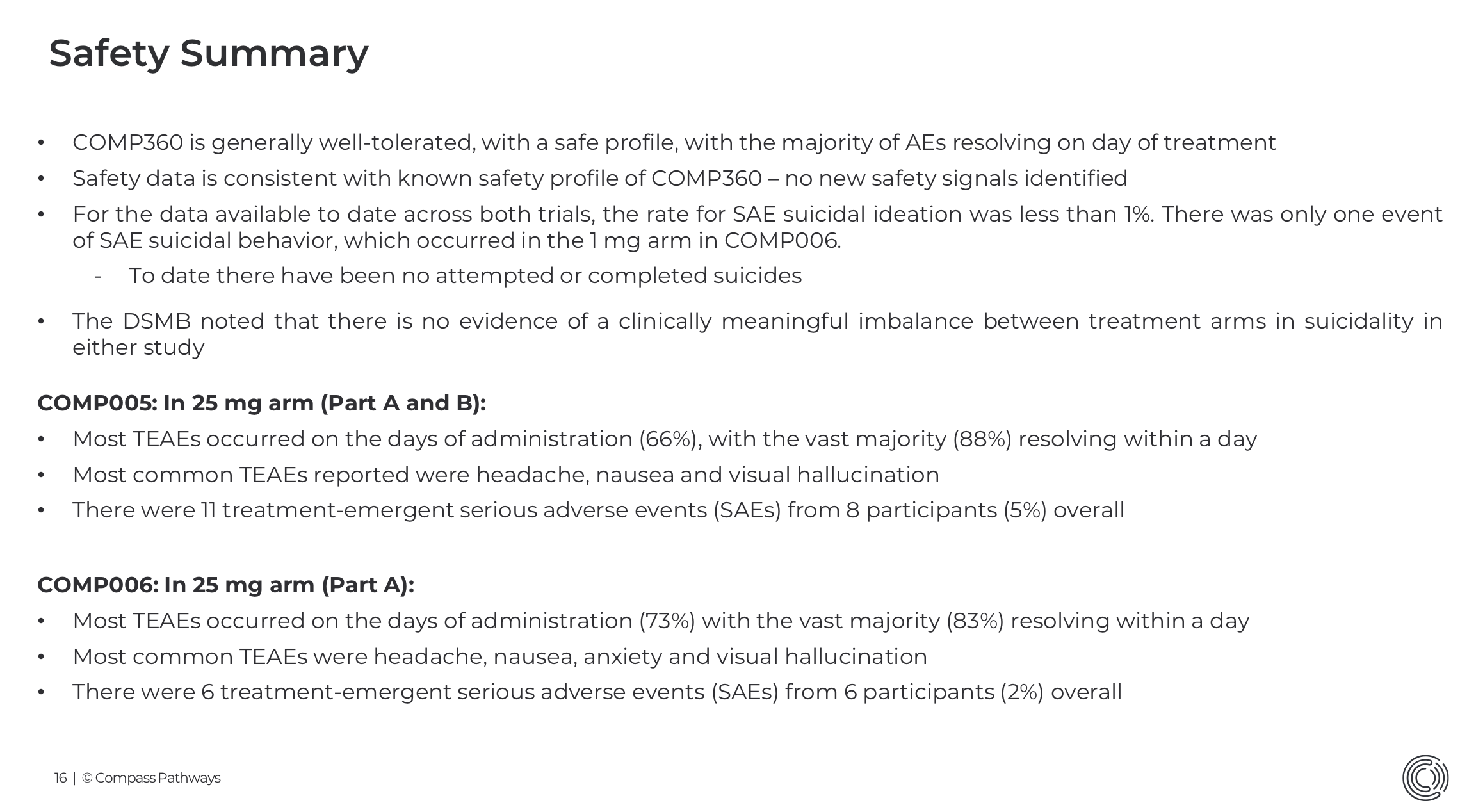
My point here was that whether one considers the efficacy in the comp001, comp005, and comp006 studies significant or a disappointment, that efficacy “delta” is now known (also by the FDA). If you have followed Makary’s statements, it seems that a MADRS delta of -3.6 and -3.8 points at the Phase 3 level is at least not a factor that would cause a marketing authorization to be denied. Clearly, the path to approval is being paved by the head of the FDA, and political and other guidance likely affects the perspective from which the FDA views the application data (even if it theoretically shouldn’t). The Comp005 26-week data was positive regarding the durability of efficacy; comp006 results will be seen at the beginning of Q3. I find it hard to believe it would be so bad that it would change the overall picture anymore. So far, about a thousand patients have been dosed and most have been followed for the entire follow-up period; the IDMC (Independent Data Monitoring Committee) has not observed a difference in suicidality between the groups or, based on its statement, other serious adverse effects.
In my thinking, the ground on which the FDA could justify not granting marketing authorization is precisely this impossibility of proper blinding, and thus the impossibility of saying for sure what the relationship is between the pharmacological effect and the effect of efficacy expectation. I was somewhat worried about this before Saturday, because it emerged a couple of months ago that Compass was on that first FDA/Makary commissioner’s national priority voucher list (a new system where drugs considered nationally most significant can be approved in a few weeks from filing), but the White House removed Compass from the list just a few hours before it was published. I thought that if for political reasons they don’t want to grant marketing authorization to a “drug” in an election year, a justification for refusal can certainly be found.
But now, after watching the ceremony, where it was implied (without naming the company) that Compass will receive that CNPV (Commissioner’s National Priority Voucher), I am no longer worried about the project being sabotaged for political reasons. I also believe—since I think there are good grounds to approve the application—that this political will and the will of the FDA leadership will lead to the blinding problem not being examined from a harshly realistic angle. The issue has been quite well understood in both psychedelic research and the FDA for a long time. Or if an advisory committee is formed, it will be assembled in such a way that the matter is viewed largely from the perspective of psychedelic research rather than a “nihilistically puritanical” perspective.
I’m rambling on. In any case, I believe the marketing authorization will come. I believe that after that, not only on the initiative of doctors, but from patients seeking help for treatment-resistant (and probably other) depression, there will be interest and requests to try this form of treatment. It’s worth watching that EO (Executive Order) press conference. From a scientific point of view, it is cringe-inducing, but if even a fairly significant proportion of people are prone to thinking in the same vein about psychedelic treatments versus traditional antidepressants, and if political permission and “folklore” providing ingredients for a good story lead to increasing visibility in the media, this could very quickly become a blockbuster!
People like to listen to stories, and the experiences described by patients from psychedelic therapy versus SSRIs are completely different, even if—reducing it to MADRS differences—one might think that some kind of similar treatment is involved (Of course, there are also infrastructure-related constraints, but the infrastructure will grow if there is demand; additionally, insurance coverage is a key issue, and I can’t say how much political will can contribute to this?)
First of all, @JusaVaan, thanks for the “field promotion”; I really appreciate that it crossed your mind that the OP might be a psychiatrist I actually graduated on March 4, 2026, from the University of Helsinki (Licentiate of Medicine, LL) and received my license on March 17, 2026, from the LVV (National Supervisory Authority for Welfare and Health) — I’ll be submitting my application for psychiatry residency/specialization training this fall. Currently, I’m working as a ward physician in the mood disorders ward of a certain hospital. I’ve had a very strong interest in mood disorders for a long time, and unfortunately, from the perspective of TRD, I also have experience from the other side of the table — that’s why the subject is so important to me and why I want to build my career in that field.
I apologize for the outright carelessness in certain phrasings yesterday; the OP was clearly far too tired yesterday. Regarding TRD, @JusaVaan: you’re right, I should have been writing all along that I’m talking about antidepressant augmentation (and why not also, for example, antipsychotic or lithium augmentation), or alternatively, a specific study design where, after a second failed drug trial, a switch to a third antidepressant is attempted, or then the treatment method being studied (so in this case, this would be a valid study scenario only for those patients where the failed number of treatment attempts = 2).
According to my own limited understanding, the current situation regarding psychedelics is such that a difference in efficacy compared to antidepressants in non-treatment-resistant situations hasn’t been demonstrated, but regarding TRD, it’s still hard to say one way or the other based on the research data. And this probably partly influences, among other things, Isometsä’s perhaps slightly negative-realistic interpretation of the situation.
Regarding MADRS: I agree with @JusaVaan that in reality, when moving into the clinical world and away from drug trials, MADRS score reductions aren’t the most essential metric. What’s essential in these drug trials would be to get the MADRS score reductions on the right side of the decimal point, and thereby provide the regulatory authority with sufficient evidence of efficacy. However, MADRS is the best of the available forms for assessing the efficacy of depression treatment as objectively as possible; BDI-21 and PHQ-9 leave the assessment of the situation entirely to the patient (unless a clinician fills them out, which is extremely rare), which likely presents several issues in this context.
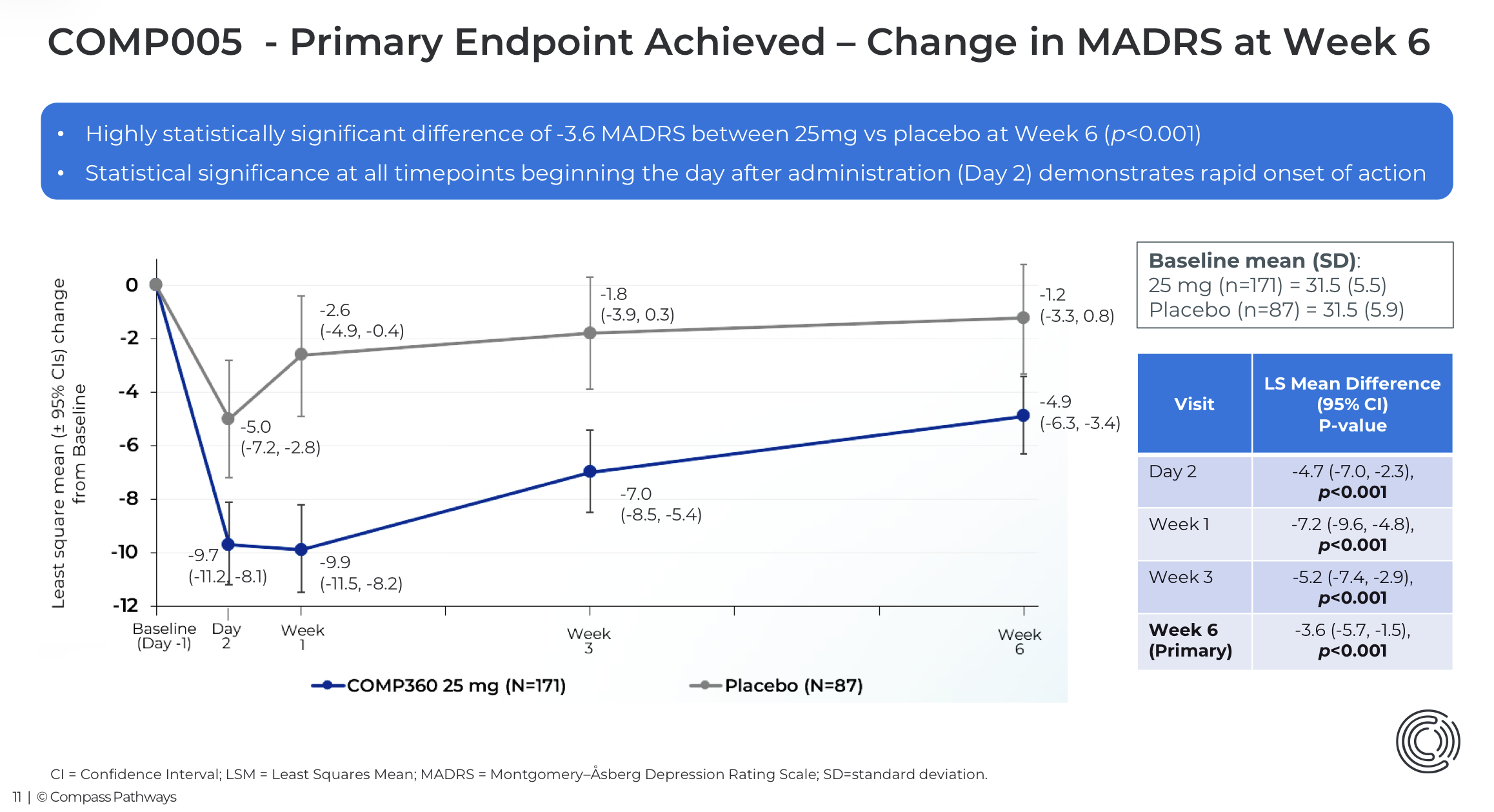
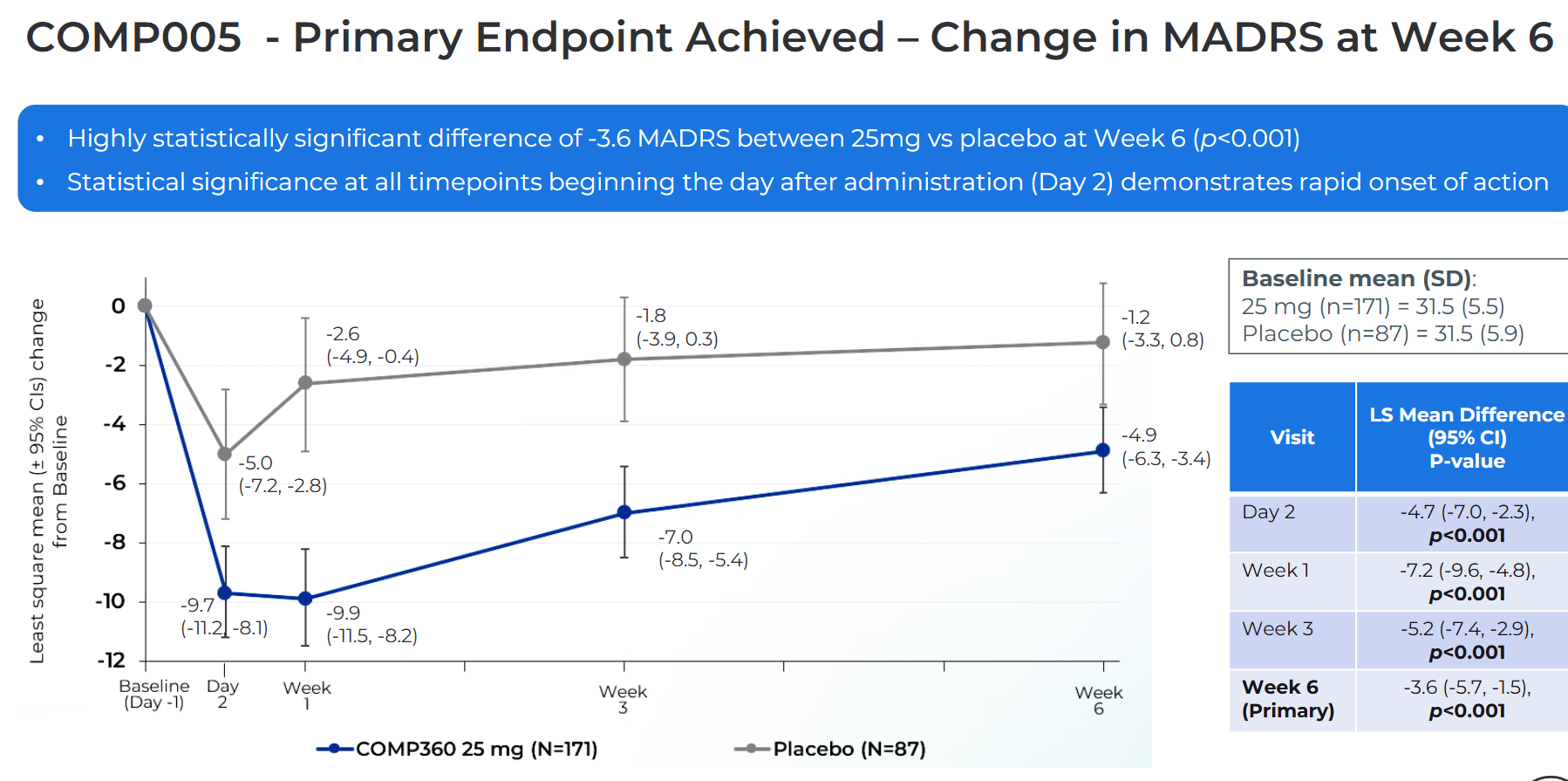
So, Compass has conducted two Phase 3 trials, one of which (comp005) compared psilocybin 25 mg vs. placebo and the other (comp006) 25 mg vs. 10 mg vs. 1 mg, with two doses administered 3 weeks apart. Pohjolan Eka posted graphs of the primary endpoints above, which also show the magnitude of the placebo response.
According to Compass’s communication, placebo-controlled data is essential especially for demonstrating safety, and this comp006 (like comp001) aims to overcome the functional unblinding problem.
(However, it seems that in newer studies by other companies, they are returning to placebo comparisons, e.g., ATAI/pbl-003, so it might be that the FDA is starting to accept that full and true blinding in these studies is simply not possible to achieve?)
By the way, I have written quite a bit about Compass and other players in the field in the “Searching for Top Medical Technology Products” (Lääketieteen teknologisia huipputuotteita etsimässä) thread over the last year or so (?), if anyone happens to be interested in previous reflections. I can’t move everything here, and this thread is intended to be CMPS-specific, but it’s good to understand the competitive landscape; CMPS is not the only player, although it has the potential for the first FDA approval.
One thing that has perhaps been highlighted less in our Compass discussions, in addition to the delta, is the efficacy of the placebo group in COMP 005, where there was a true placebo; the MADRS at week 6 was -1.2. That is quite low for a placebo response. This raises the question of whether the subject realizes they have received a placebo because they did not experience a trip effect, meaning are we seeing a nocebo effect? This would, in itself, cause an otherwise decent delta to be inflated.
If we look at the placebo response rates in some other TRD (Treatment-Resistant Depression) trials, they are much higher than the -1.2 observed in COMP 005.
The stock price is currently undergoing some kind of hype effect fueled by Trump. If we could also get a Kardashian or similar to speak about psilocybin treatment, then voila. However, I am now leaning towards the bear camp; except for momentum trading, considering the possibilities of falling foul of the FDA, the risk-reward is now against the investor following the price increase.
How can that be? To me, it seems the FDA is involved in the game, getting the first psychedelic therapy through in a few months. It’s been clear to everyone (including the FDA) for years that proper blinding is impossible with high-dose psychedelics. The FDA (Makary) knows very well what kind of data is coming for evaluation, so why on earth would they put on such a show if in a few months they’d scrutinize the data through an unreally realistic lens, when there are “honest” opportunities for another approach (e.g., an advisory board with experts from psychedelic research)?
Isn’t Joe Rogan good enough already?
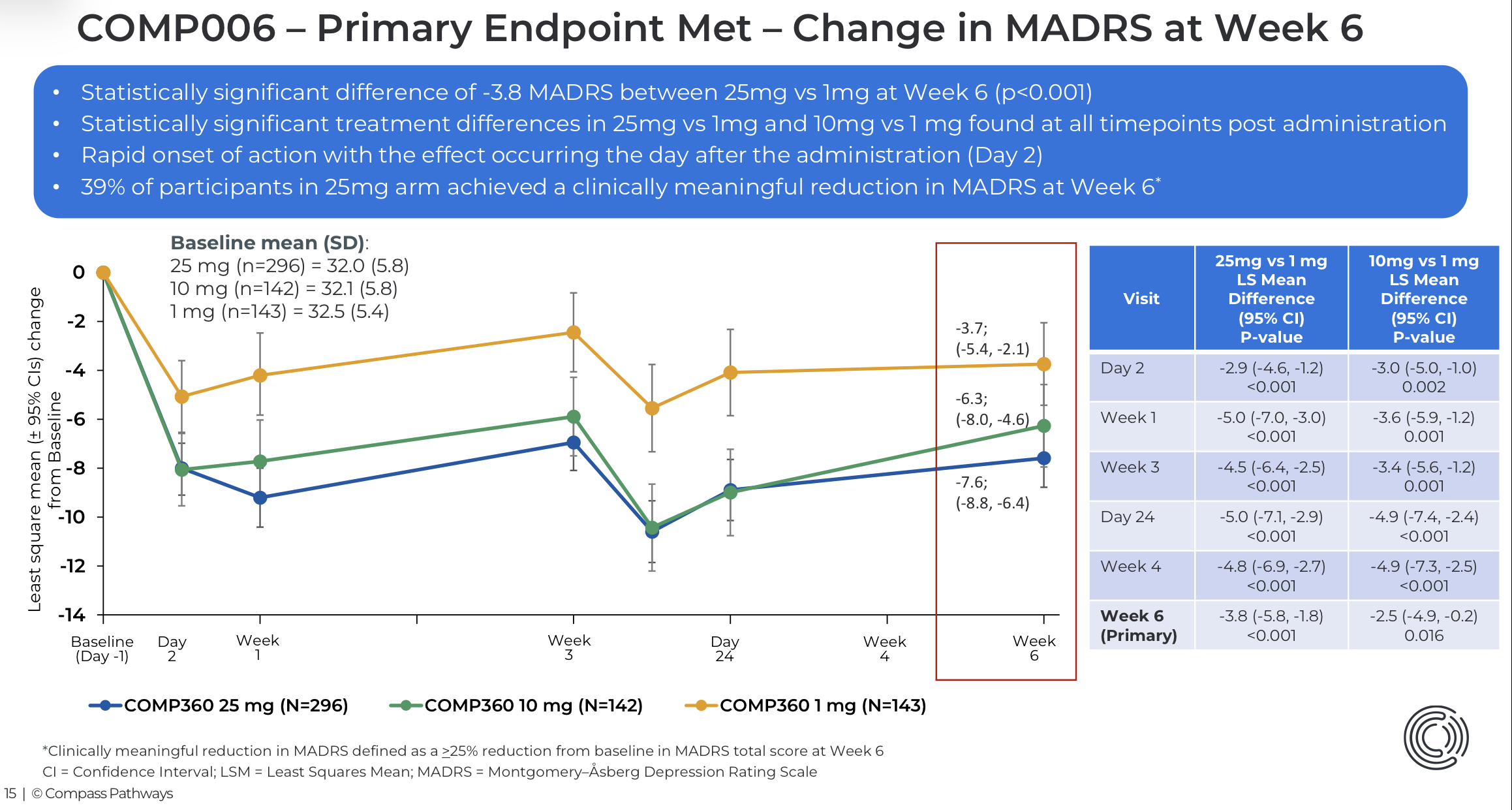
Isn’t COMP006, where efforts have been made to mitigate the blinding problem, already quite good? The 1 mg dose, which served as a placebo, showed a -3.7 point reduction.
I haven’t been following that closely lately, but are there any other indicators of the FDA being on board besides Makary’s obvious positive stance? He obviously isn’t making the decisions directly, but he could certainly use all the means at his disposal (blackmail, threats, bribery :D) against FDA officials… Trump used an executive order to speed up decision-making, but surely even he can’t influence the requirements for scientific evidence… right…? (insert Anakin and Padme meme here)
So Makary, without mentioning Compass by name, practically promised Compass a Commissioner’s National Priority Voucher, and it would have been taken care of already if someone hadn’t blocked it at the last minute last fall.
Of course, expedited processing of a marketing authorization application is still a matter of reviewing scientific data, but that voucher reflects a statement of intent, and no psychedelic can be approved if absolutely effective blinding is a requirement—which is why I think it would be strange to set the stage for this so strongly if the matter were to fail over this known “basic problem” inherent to any psychedelic research, which could also be considered a feature of the treatment.
Apologies for the multiple edits to the previous post, I was adding points there…
The desired state clearly seems to be there. Whether it will materialize as hoped is so much a matter of subjective evaluation that it’s hard to say anything. My coin toss usually lands on the opposite side to the FDA.
However, it’s good to know that there is a precedent regarding the significance of desired states: aducanumab was pushed through for Alzheimer’s approval despite the evidence being absolutely rubbish. I think I may have mentioned this before. There are probably other examples, but that one always comes to mind for me.
Thanks for sharing your thoughts anyway, and for the discussion. It’s a fact that you have more experience with this coin toss, so it’s possible that I believe my own thesis too strongly (this is a disclaimer for others following the thread!)